CBHL has a rich history of convening influential leaders via annual Summits, serving as incubators of national change. Given the uncertainty due to COVID-19 in 2020, we created an innovative way for leaders to gather using new technology. Instead of meeting in-person, we delivered the same nationally recognized speakers, thought provoking content and meaningful dialogue over a series of weeks – all within in a flexible virtual format consisting of highly engaging, interactive events.
We examined partnerships whose collaboration resulted in real outcomes as we learned from community initiatives across the country. Featured partnerships demonstrated improvements in community relationships resulting in measurable impacts to community health, for different populations, using different approaches to multi-sector collaboration.
Specifically, attendees:
- LEARNED different approaches (models) of engaging multi-sector, community-based collaboration
- CONSIDERED how these models can be used to tackle different types of complex behavioral health challenges in communities
- CLARIFIED key characteristics and pros/cons of each approach
- CONNECTED with colleagues and build new relationships
- IDENTIFIED how these models can be applied to address a challenge their community is facing
Click on each banner below for session descriptions.
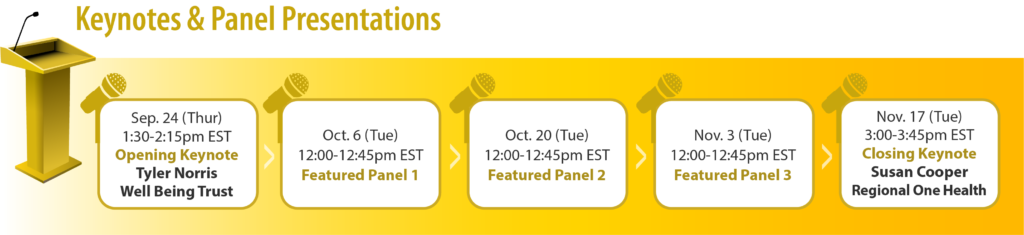
We were proud to feature Tyler Norris and Susan R. Cooper as our opening and closing keynote speakers! Click here to learn more about them.

Tyler Norris, MDiv

Susan R. Cooper, MSN, RN, FAAN
Click here to learn more about our panelists!
Panel & Interactive Session 1 | Partnerships in the Community: Imperative to Keeping the PACE (Philadelphia, PA)
- Kurt August, Assistant Director Diversion & Deflection, Managing Director’s Office of Criminal Justice
- Dana Careless, Executive Coordinator for Philadelphia Department of Behavioral Health and Intellectual disAbility Services (DBHIDS)
- Eduardo “Eddie” Collazo, Director, Multicultural Affairs, Philadelphia Department of Behavioral Health and Intellectual disAbility Services (DBHIDS)
- Nick Fagan, Community Member
- Crystal Yates, Deputy Commissioner, City of Philadelphia Emergency Medical Services
Panel & Interactive Session 2 | The Beginning of the End: Leveraging Partnerships, Data, and Lived Expertise to Effectively End Youth Homelessness (Austin, TX)
- Liz Schoenfeld, PhD, Chief Research & Evaluation Officer for LifeWorks
- Erin Whelan, Senior Division Director for Housing and Homeless Services at LifeWorks
- Bree Williams, Director of Community Housing for the Ending Community Homelessness Coalition (ECHO)
- Lyric Wardlow, Founding Member of the Austin Youth Collective
- Maryam Zia, Diversion Program Services Coordinator for LifeWorks
Panel & Interactive Session 3 | Douglas County Mental Health Initiative: A Unique Community Partnership (Douglas County, CO)
- Barbara Drake, Deputy County Manager in Douglas County
- Douglas Muir, LCSW, CACIII, MBA, Behavioral Health Service Line Director for Centura Health
- Jenn Conrad, LCSW, CCM, Director of Clinical Services with Signal Behavioral Health Network
- Captain Kevin B. Duffy, #89-05 Douglas County Sheriff’s Office Investigation Division Commander
- Laura Ciancone, MPH, Mental Health Initiative Coordinator for Douglas County