Crossing the Quality Chasm: Translating the Institute of Medicine Report for Behavioral Health
March 13-16, 2002
Eldorado Hotel & Spa Santa Fe, NM
Allen S. Daniels, LISW, Ed.D., Program Chair
Hubert A. Mintz, III (Ting), Co-Chair
Introduction
In 2001 the Institute of Medicine (IOM) published, Crossing the Quality Chasm. This report of the Committee on the Quality of Health Care in America followed the 1999 report To Err is Human: Building a Safer Health System. Taken together, these reports identify critical problems with the American health care systems and begin to lay out a strategic direction for the redesign of systems for the 21st century. Over the past several years, it is increasingly clear that the work of the Committee on The Quality of Health Care in America has made a substantial contribution to the evolving health policy debate on the reform of health systems. These reports have gained widespread acceptance and there is interest in using them as blueprints for change.
However, attention to specific issues germane to the delivery of services for mental health and addictive disorders has been limited. This failure to address behavioral healthcare has left a gap in the comprehensive scope of these reports and the agenda for systems change. The importance of mental health and addictive disorders and their impact on health status and health systems are too significant to be left unattended.
In an effort to speak to this gap, the American College of Mental Health Administration (ACMHA) elected to focus the2002 Summit on the “translation” of the Quality Chasm report for the mental health and addictive disorders field. As a small multidisciplinary leadership organization recognized for its success as a neutral convener in the field , the College is in an ideal position to undertake this effort.
ACMHA has an established track record of addressing the pressing issues facing the behavioral healthcare field at its annual Summits. These meetings are working forums that have produced summary reports and have spawned a series of project initiatives. Previous Summit topics and projects have considered:
- The development of practice guidelines for the behavioral health field;
- The crisis in training and workforce development for behavioral healthcare;
- The development and promotion of common performance measures for the behavioral healthcare field; and
- Financing strategies for quality and performance in behavioral healthcare
The ACMHA 2002 Summit convened March 14-16, 2002 in Santa Fe, New Mexico. The ninety-two attendees represented diverse stakeholder interests in the field and included leaders from public and private behavioral healthcare systems, administrators and service providers of child/adolescent, adult, elderly, mental health, substance abuse care, consumers, persons in recovery, family members, academicians/ educators, researchers, and other professionals.
Process
In order to attempt a translation of the IOM report, the ACMHA Summit constructed a framework to involve participants in the assessment, evaluation and analysis of the IOM reports from a behavioral healthcare perspective. The format included both didactic presentations and small working group sessions to examine specific aspects of the Quality Chasm report. Data from the working groups was collected for qualitative analysis.
All of the participants were provided an orientation to the “IOM Quality Chasm Report.” The participants were then randomly assigned to six working groups. Each of the groups met twice over two days for a total of four hours. The groups shared a common task for both day one and day two assignments.
The first day assignment was for each of the groups to conduct a Strengths, Weaknesses, Opportunity, and Threat Analysis (SWOT). Each group was randomly assigned two “Aims” from the “IOM Quality Chasm Report”. None of the groups had the same pair of aims. Data from the discussion for each group was compiled and submitted for analysis. Following the first group session was a one hour debriefing for group leaders which included a review of the day one process and results, as well as planning for the second group assignment.
The second day of the summit began with a facilitated discussion of the group experiences prior to the second small group meeting. Participants were also provided with a review of current initiatives that influence the future of behavioral healthcare. This included material from the Substance Abuse and Mental Health Administration’s current agenda, a report from the National Institute of Mental Health on new funding initiatives, the Surgeon General’s report on Mental Health, and consumer led initiatives.
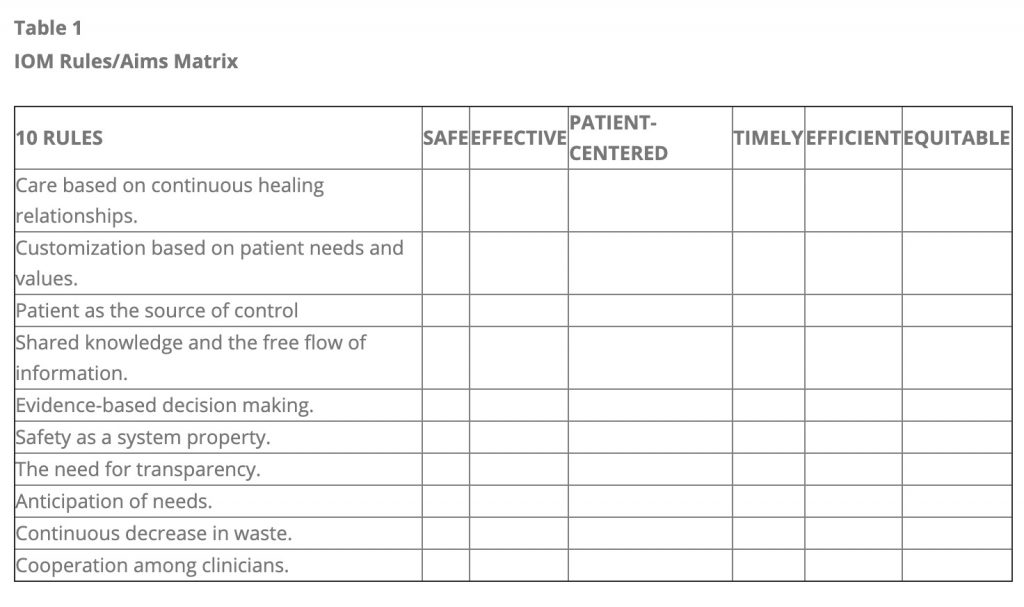
The second small group session was designed to incorporate the work of the first session on the specific aims with an added focus on the Quality Chasm report’s ten rules. Group membership and leadership remained consistent for both sessions. Each group was assigned five of the ten rules from the “Quality Chasm Report”. The rules were assigned so that each of the aims would have a corresponding match with each of the ten rules. Leaders and participants were provided a matrix that incorporated the six aims and ten rules. (See Table 1 below).
At the conclusion of the second group session, the leaders re-convened for debriefing which focused on developing presentation of materials for a final summation session with the Summit participants. A summary presentation was made by each group and there was a general response discussion by all participants.
Preliminary Findings and Data Analysis
The participants of the ACMHA Summit met on the last day to discuss their experiences and make recommendations for future directions. The overwhelming consensus of the participants was very favorable. In general, they found that the Qualty Chasm Report was very applicable to the concerns and needs of the behavioral healthcare field. Their more specific recommendations are detailed in the next steps section of this report.
The facilitated group sessions provided a a wealth of information: a consensus report of the participants, and the accumulated data which are available for future analysis. The combination of these provides a framework for the future of this ACMHA initiative. The findings from each of the working groups are rich with analysis and examples from the participants, including a SWOT analysis for each of the six IOM Quality Chasm aims, representing a cogent summary of the application of the aims for behavioral healthcare and a summary of the application of these concepts to the field. Because there were multiple groups examining each aim, there is substantial depth and breadth of resources included in each analysis. These data are further enriched by the vast spectrum of experience of the participants.
The data from the SWOT analysis of each of the six aims have also been used in an examination of the ten rules. The result is a matrix that considers all of the aims and their relationship to each of the ten rules. Together, this level of data can provide a valuable resource for both further translating the IOM report for behavioral healthcare as well as addressing the strategic planning goals of the ACMHA Quality Chasm initiative.
Next Steps
The overwhelming consensus of the participants of the ACMHA 2002 Summit was that the IOM Quality Chasm framework is immediately relevant and applicable to the concerns of behavioral health systems of care and policy. In addition, the participants affirmed the need to translate the material to the specific behavioral healthcare issues field and to address its integration into the larger general healthcare systems. Furthermore, the participants acknowledged and endorsed the IOM paradigm as a strategic planning blueprint for the redesign of the behavioral healthcare system.
The Summit attendees and College leaders concluded by endorsing this work as an ongoing ACMHA initiative. This effort was seen as a natural continuation and extension of past College efforts, described earlier, to address key quality concerns for the mental health and addictive disorders field.
Based upon the endorsement of the ACMHA members and Summit attendees for the ongoing work of the Quality Chasm Initiative, several next steps are planned. These include:
- meeting with the Institute of Medicine to explore collaborative opportunities for the work of this initiative;
- meeting with other policy and payer stakeholder groups (e.g. SAMHSA, NASMHPD, CMS) to explore collaborative initiatives;
- meeting with and presenting proposals for resource development to funding sources;
- analysis and reporting of the Summit data and dissemination of findings; and
- development of best-practice model programs and field testing of results.
Table 1
IOM Rules/Aims Matrix